
Both STK11 (also called LKB1) and KEAP1 mutation occur in about 17% of Non Small Cell Lung Cancer (adenocarcinomas), respectively, and correlates with poor outcome with immune checkpoint inhibitors or immune checkpoint inhibitors plus chemotherapy. KRAS is frequently comutated with STK11, KEAP1, and TP53 and these subgroups confer different prognostic outcomes. Within the KRAS mutated population, STK11 and/or KEAP1 mutations are associated with inferior Overall Survival and Progression Free Survival across treatments, compared with STK11-wild type and/or KEAP1-wild type. It appears that anti PD-1/anti-PD-L1 immune checkpoint inhibitors in combination with anti-angiogenic agent and chemotherapy is an efficacious first-line treatment in metastatic NSCLC subgroups with KRAS mutations co-occurring with STK11 and/or KEAP1 or TP53 mutations and/or high PD-L1 expression.
Tag: Lung Cancer: Non-Small Cell
Lobar or Sublobar Resection for Peripheral Stage IA Non Small Cell Lung Cancer
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 21% of all cancer deaths. The American Cancer Society estimates that for 2023, about 238,340 new cases of lung cancer will be diagnosed and 127,070 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
Low Dose CT (LDCT) screening for lung cancer resulted in a 20% reduction in mortality In the National Lung Screening Trial (NLST). The USPSTF expanded the criteria for lung cancer screening in 2021 and recommended annual screening with Low-Dose CT for adults aged 50-80 years who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years. Approximately 15% of patients present with early stage (T1-2 N0) disease, and these numbers are likely to increase with the more rigorous implementation of lung cancer screening programs.
Surgical resection is the primary treatment for approximately 30% of patients with NSCLC who present with early Stage (I–IIIA) disease. Pneumonectomy is rarely performed due to unacceptably high mortality rate. Lobectomy has been the standard of surgical care for patients with clinical T1N0 NSCLC since the mid 1990s. This was based on the results of a randomized trial comparing Lobectomy with Sublobar resection in patients with clinical T1N0 NSCLC. In this trial, the frequency of local recurrence was three times higher with Sublobar resection compared with Lobectomy, and lung cancer-related mortality was 50% higher with Sublobar resection.
Sublobar resection includes Wedge resection and Segmentectomy. In Wedge resection, the lung tumor is removed with a surrounding margin of normal lung tissue, and is not an anatomical resection. Segmentectomy, unlike Wedge resection, is an anatomical resection that usually includes one or more pulmonary parenchymal segments with the dissection of intraparenchymal and hilar lymph nodes. Advances in imaging as well as staging by means of mediastinoscopy, and routine intraoperative lymphadenectomy has enabled the identification of small, peripheral NSCLCs for which Sublobar resection was potentially appropriate. Sublobar resection was considered a “compromise operation” in selected high risk patients with early stage lung cancer. With the approval of lung cancer screening in high risk individuals and subsequent detection of small tumors, Sublobar resections have been on the rise and may be the preferred surgical option, even in good-risk patients, in many institutions. Sublobar resection preserves pulmonary function and leaves open more treatment options for NSCLC patients, who remain at high risk for metachronous primary NSCLC, following curative intervention for their first NSCLC.
With the implementation of CT-based lung cancer screening recently, lung cancers are likely detected at a very early stage (T1a-bN0; 2 cm or less, node negative tumors). Further, Adenocarcinoma now is the most frequent histologic subtype of lung cancer and present as peripherally located tumors. Advances in preoperative staging such as endobronchial ultrasonography, have improved patient selection for treatment. Majority of surgical resections are now performed by means of video or robotic-assisted thoracic surgery. This has improved postoperative outcomes, with significant reduction in perioperative morbidity, mortality and median length of hospital stay after either Sublobar resection or Lobectomy.
The authors in this study reported the results of a randomized international trial comparing Sublobar resection (wedge resection or segmentectomy) with Lobectomy, in patients with clinical Stage IA NSCLC, with a tumor size of 2 cm or less. Cancer and Leukemia Group B (CALGB) 140503 was a multicenter, international, randomized, noninferiority, Phase III trial, involving patients with NSCLC clinically staged as T1aN0. In this study, a total of 697 patients, after intraoperative confirmation of node-negative disease, were randomly assigned to undergo either Sublobar resection (N=340) or Lobar resection (N=357). Of the 340 patients assigned to Sublobar resection, 201 (59.1%) underwent wedge resection and 129 (37.9%) underwent an anatomical segmental resection. Wedge resection was allowed in the current trial as it is the most frequently practiced method of Sublobar resection in North America and Europe and its inclusion would make the trial more representative of a “real world” setting. The median patient age was 68 years. Approximately 50% of patients had tumor size 1.0-1.5 cm, 40% had tumor size 1.5-2.0 cm, and two thirds of the patients had Adenocarcinoma histology. Over 90% of the patients were current or former smokers. The Primary end point was Disease-Free Survival (DFS), defined as the time between randomization and disease recurrence or death from any cause. Secondary end points included Overall Survival (OS), locoregional and systemic recurrence, and pulmonary functions.
After a median follow up of 7 years, Sublobar resection was noninferior to Lobar resection for DFS (HR for disease recurrence or death=1.01). The 5-year DFS was 63.6% after Sublobar resection and 64.1% after Lobar resection. The Overall Survival after Sublobar resection was similar to that after Lobar resection (HR for death, 0.95). The 5-year OS was 80.3% after Sublobar resection and 78.9% after Lobar resection. No substantial difference was seen between the two groups in the incidence of locoregional or distant recurrence. At 6 months postoperatively, pulmonary functions favored the Sublobar resection group.
It was concluded that Sublobar resection by either anatomical segmentectomy or wedge resection, for patients with peripheral NSCLC with a tumor size of 2 cm or less and pathologically confirmed node-negative disease in the hilar and mediastinal lymph nodes, was non inferior to Lobectomy, with respect to Disease Free Survival and with similar Overall Survival, and is an effective management approach for this subgroup of patients with NSCLC.
Lobar or Sublobar Resection for Peripheral Stage IA Non–Small-Cell Lung Cancer. Altorki N, Wang X, Kozono D, et al. N Engl J Med 2023; 388:489-498
FDA Approves Adjuvant KEYTRUDA® in NSCLC Irrespective of PD-L1 Expression
SUMMARY: The FDA on January 26, 2023, approved KEYTRUDA® (Pembrolizumab) for adjuvant treatment following resection and platinum-based chemotherapy for Stage IB (T2a ≥4 cm), II, or IIIA Non-Small Cell Lung Cancer (NSCLC). Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 21% of all cancer deaths. The American Cancer Society estimates that for 2023, about 238,340 new cases of lung cancer will be diagnosed and 127,070 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
The 5-year survival rate for patients diagnosed with lung cancer in the US is about 25%, which is a significant improvement over the past 5 years, in part due to earlier detection from lung cancer screening, reduction in smoking, advances in diagnostic and surgical procedures, as well as the introduction of new therapies. However, the 5-year survival rate remains significantly lower among communities of color at 20%. Early detection and screening remain an important unmet need, as 44% of lung cancer cases are not found until they are advanced. In the US, only 5.8% of those individuals at high risk were screened in 2021.
Surgical resection is the primary treatment for approximately 30% of patients with NSCLC who present with early Stage (I–IIIA) disease. These patients are often treated with platinum-based adjuvant chemotherapy to decrease the risk of recurrence. Nonetheless, 45-75% of these patients develop recurrent disease. There is therefore an unmet need for this patient population.
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. By doing so, it unleashes the tumor-specific effector T cells, and is thereby able to undo PD-1 pathway-mediated inhibition of the immune response.
KEYNOTE-091/EORTC-1416-LCG/ETOP-8-15 – PEARLS trial is a multicenter, randomized, triple-blind, placebo-controlled Phase III trial, which compared the efficacy of KEYTRUDA® with placebo, among patients with resected NSCLC. In this study, 1,177 patients with completely resected Stage IB (T2a ≥4 cm), II, or IIIA NSCLC with negative margins, and with tumor tissue available for PD-L1 testing were included. Systematic complete or lobe-specific mediastinal lymph node dissection was recommended. In the least, the subcarinal and 1 lobe-specific lymph node must have been examined. Eligible patients had not received neoadjuvant radiotherapy or chemotherapy, had ECOG PS of 0-1, and adjuvant chemotherapy for up to four cycles was optional. Adjuvant chemotherapy could be considered for those with Stage IB disease and was strongly recommended for those with Stage II and IIIA disease. Patients were randomized (1:1) to receive KEYTRUDA® 200 mg or placebo IV every three weeks and treatment was continued until disease recurrence, unacceptable toxicity, or up to 1 year. Both treatment groups were well balanced. The median patient age was 65 years, majority of patients (68%) were male, approximately 65% of patients had nonsquamous histology, 56% of patients had Stage II disease and 86% of patients had received adjuvant platinum-based chemotherapy following complete resection. Stratification factors included disease stage, receipt of adjuvant chemotherapy, PD-L1 Tumor Proportion Score and geographic region of the world. The median duration of exposure to KEYTRUDA® was 11.7 months and 68% of patients in the KEYTRUDA® group were exposed to KEYTRUDA® for at least 6 months. The major efficacy outcome measure was investigator-assessed Disease-Free Survival (DFS). An additional efficacy outcome was Overall Survival (OS).
The trial met its Primary endpoint, demonstrating a statistically significant improvement in DFS in the overall population. In patients who received adjuvant platinum-based chemotherapy following surgical resection, KEYTRUDA® reduced the risk of disease recurrence or death by 27% (HR=0.73) versus placebo, regardless of PD-L1 expression. For patients who received adjuvant chemotherapy, median DFS regardless of PD-L1 expression was 58.7 months in the KEYTRUDA® group versus 34.9 months in the placebo group. In an exploratory subgroup analysis of the 167 patients who did not receive adjuvant chemotherapy, the DFS Hazard Ratio was 1.25. Overall survival Data were not mature.
It was concluded that these data support the benefit of KEYTRUDA® as a new adjuvant immunotherapy treatment option, for early-stage NSCLC following complete resection, and if indicated, adjuvant chemotherapy, regardless of PD-L1 expression.
EORTC-1416-LCG/ETOP 8-15 – PEARLS/KEYNOTE-091 study of pembrolizumab versus placebo for completely resected early-stage non-small cell lung cancer (NSCLC): Outcomes in subgroups related to surgery, disease burden, and adjuvant chemotherapy use.O’Brien M, Paz-Ares L, Jha N, et al. DOI: 10.1200/JCO.2022.40.16_suppl.8512 Journal of Clinical Oncology 40, no. 16_suppl (June 01, 2022) 8512-8512.Published online June 02, 2022.
EGFR Exon 20 Insertion Mutations – These Are NOT Your Common EGFR Mutations


Written By: David M. Waterhouse, MD, MPH & Anita Koshy, MD
This promotional educational activity is brought to you by Janssen Biotech, Inc., and is not certified for continuing medical education.
Dr. Waterhouse is a paid consultant writing on behalf of Janssen Biotech, Inc., and must present this information in compliance with FDA requirements applicable to Janssen Biotech, Inc.
It is estimated that approximately 237,000 people in the US will be diagnosed with lung cancer in 2022. Despite advancements in standard-of-care treatments for lung cancer, this disease remains the leading cause of cancer death in both males and females.1 Nonetheless, the burgeoning number of targeted therapies for some types of lung cancer, particularly non-small cell lung cancer (NSCLC), have allowed for improvements in mortality and survival.2 As of 2022, there are ~20 targeted therapies for ~9 actionable driver mutations in stage IV NSCLC.3,4 In order to determine optimal targeted therapies, the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recommend comprehensive biomarker testing, like next-generation sequencing (NGS), for all eligible patients at diagnosis of advanced NSCLC.5
Common EGFR Mutations (Exon 19 deletion and Exon 21 [L858R] mutations)
Epidermal growth factor receptor (EGFR) is a potent oncogene commonly altered in NSCLC, and EGFR driver mutations may be found in as many as 28% of metastatic NSCLC patients.6 Tyrosine kinase inhibitors (TKIs) directed against EGFR were among the first molecular targeted agents used for treatment of advanced NSCLC.7 Initial studies of EGFR TKIs showed that patient characteristics associated with EGFR mutations, such as non-smoking status, female gender, East Asian origin, and adenocarcinoma histology suggested a greater benefit from EGFR TKIs compared with first-line chemotherapy.8 Later studies identified gene mutations that could target the kinase domain of EGFR and predicted response to such inhibitors. The variable deletions of at least 3 amino acid residues in exon 19, as well as the single point mutation leucine-858 to arginine (L858R) in exon 21, are often referred to as “common” activating EGFR mutations and represent the vast majority (90%) of all observed EGFR kinase domain mutations in NSCLC.8 (Figure 1)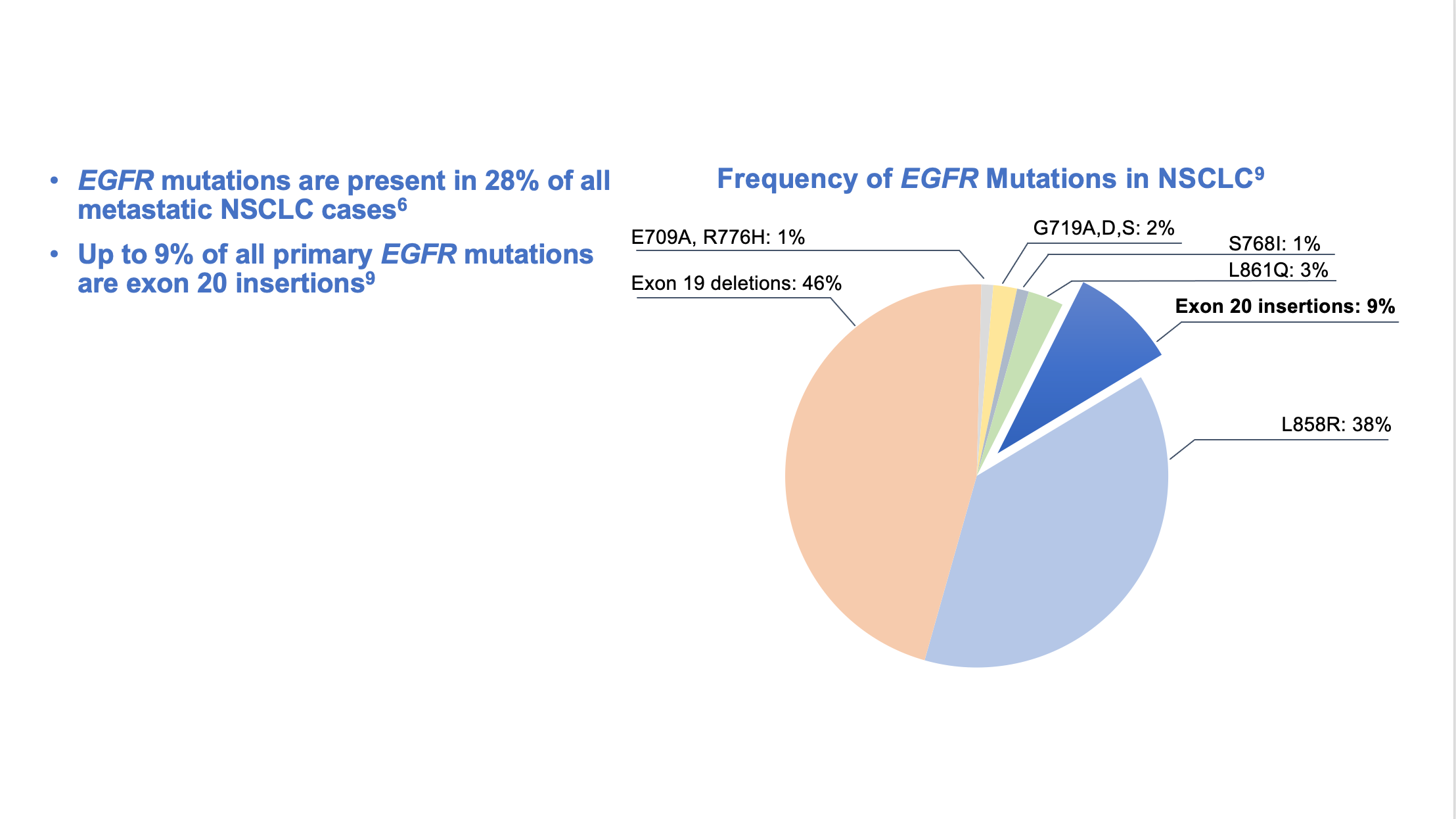
EGFR Exon 20 Insertion Mutations
Exon 20 insertion mutations are the third most prevalent type of activating EGFR mutations in NSCLC and are associated with a poor prognosis.9-11 These mutations are also enriched in women, non-smokers, Asian populations, and those with adenocarcinoma. Exon 20 insertion mutations, however, lack the key structural features that confer sensitivity of L858R and exon19 deletion mutations to first-and second-generation EGFR inhibitors. In-frame base pair insertions in exon 20 result in activation of EGFR, but, unlike the common activating EGFR mutations, they are associated with reduced affinity to most clinically available EGFR TKIs indicated for common EGFR mutations. Data are limited and variable, but multiple studies found that patients with EGFR exon 20 insertion mutations had an overall response rate of 0% to 8.7% when treated with first-, second-, or third-generation EGFR TKIs.12-16 (Figure 2)
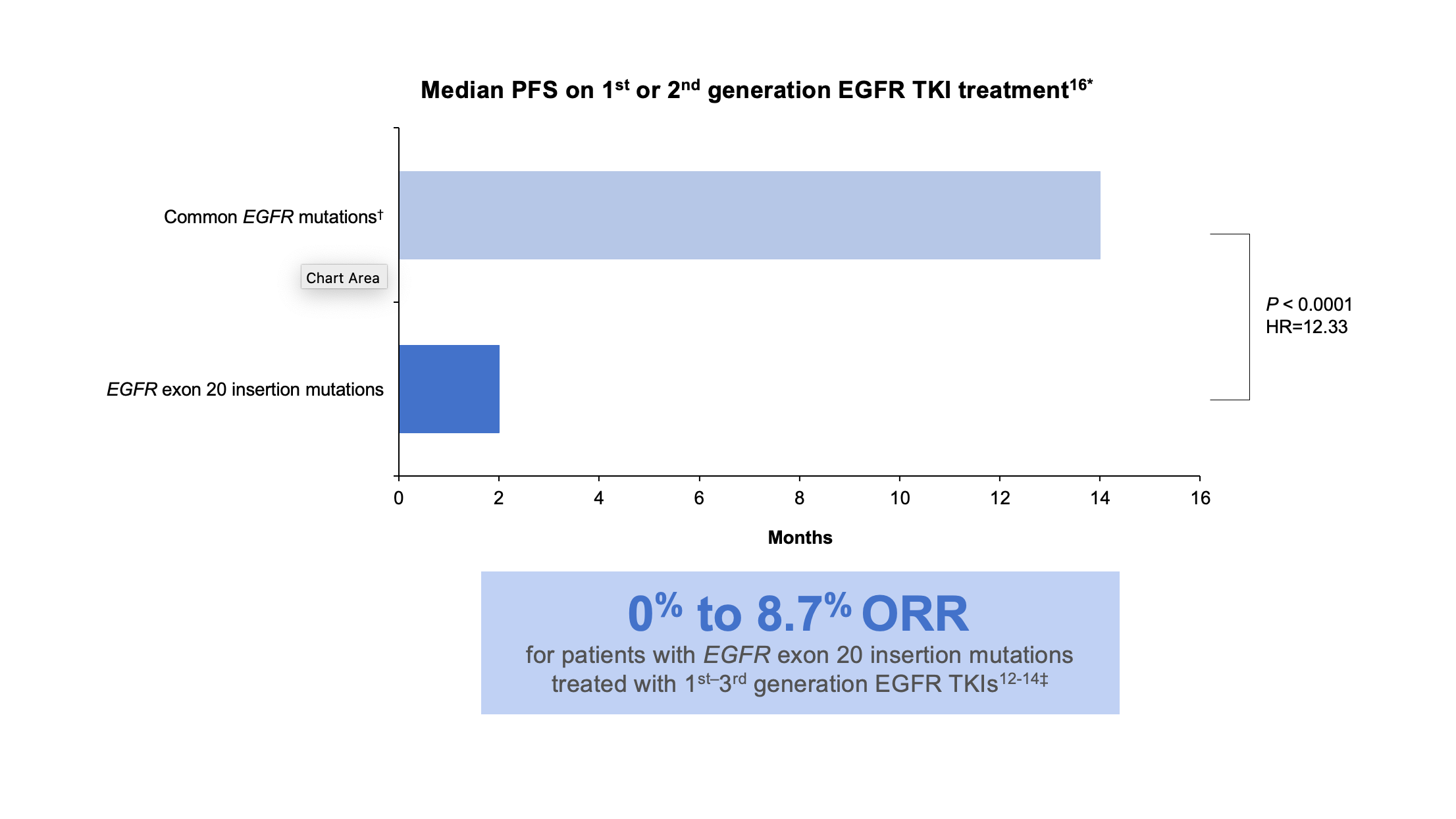
*These data were taken from a retrospective observational study.16
†Common mutations include L858R, L861Q, and exon 19 deletions.16
‡These data were taken from multiple sources: a cohort study, a prospective post hoc analysis of phase 2 and phase 3 trials, a single-center retrospective analysis, and a systematic literature review and meta-analysis.12-14
HR, hazard ratio; ORR, overall response rate; PFS, progression-free survival.
Study results also demonstrate limited efficacy of immuno-oncology (IO) monotherapy in this patient population compared to patients with wild-type EGFR. In a retrospective study using real-world data, patients with EGFR exon 20 insertion mutation-positive NSCLC were associated with a 58% increased risk of shorter time to next-line therapy after first-line IO monotherapy compared to patients with wild-type NSCLC.17
The NCCN Guidelines® do not recommend most TKIs or IO monotherapy for treating patients with mNSCLC and EGFR exon 20 insertion mutations in the first- or second-line setting. Instead, the Guidelines recommend platinum-based chemotherapy as the standard first-line treatment for NSCLC with EGFR exon 20 insertion mutations.5§
§Exceptions include p.A763_Y764insFQEA and p.A763_Y764insLQEA.5
EGFR Testing
The NCCN Guidelines recommend comprehensive biomarker testing, like NGS, prior to the initiation of first-line therapy, if clinically feasible.5 Despite that recommendation, rates of broad biomarker testing remain low, according to real-world evidence.18,19 In a retrospective observational chart review study among 3,474 patients with advanced NSCLC receiving first-line therapy in the US Oncology Network, the EGFR testing rate was found to be 70%, but comprehensive NGS testing was completed in only 42% of patients.20 Failure to order comprehensive NGS testing is particularly problematic when it comes to identifying EGFR exon 20 insertions. There are over 100 unique EGFR exon 20 insertion variants, and polymerase chain reaction (PCR) testing can miss approximately 50% of the insertions identified by NGS.21 (Figure 3)
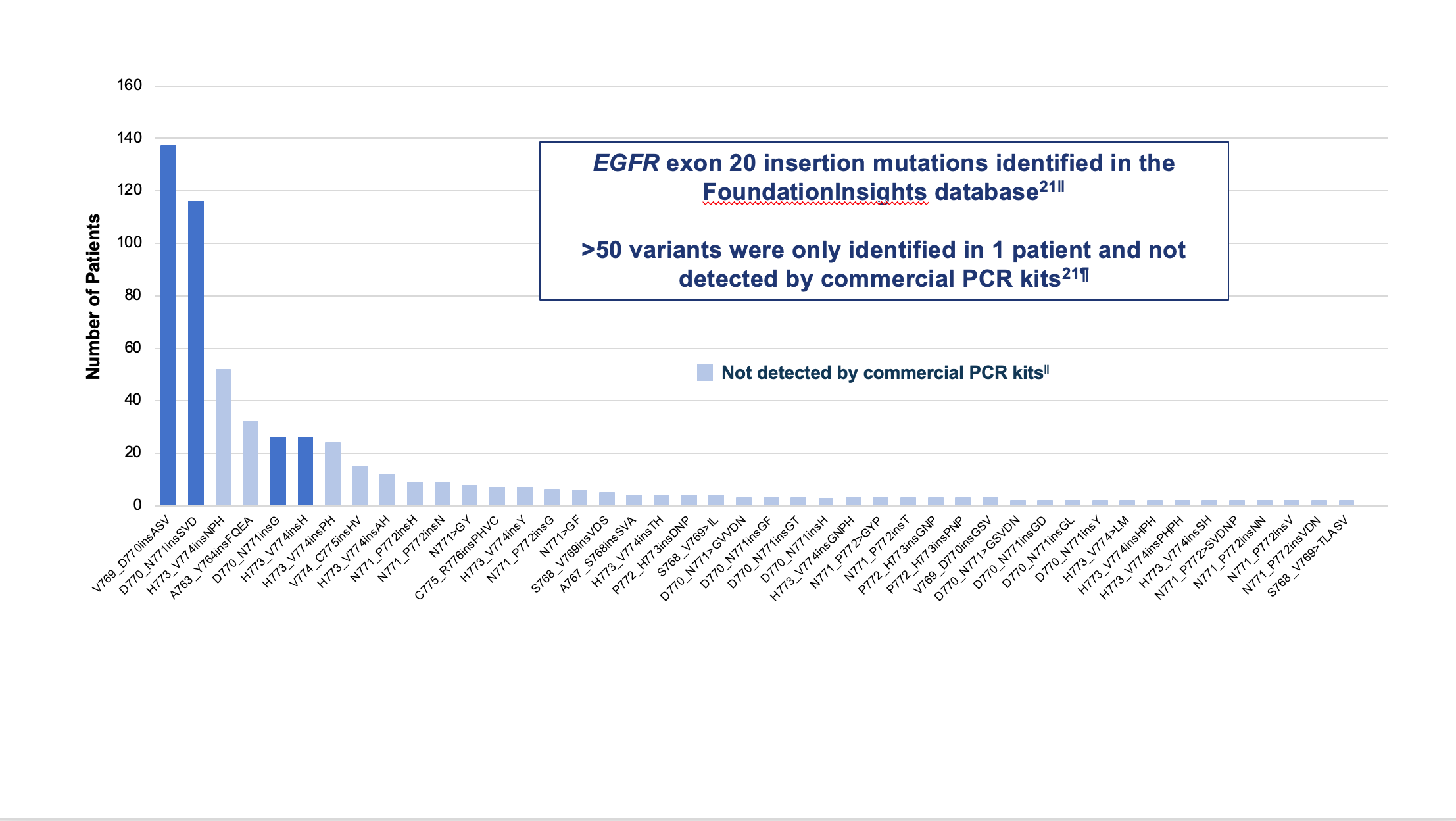
||Analysis from mutation profiles of 36,465 lung adenocarcinomas from Foundation Medicine (Cambridge, MA) FoundationInsights database, which is a database of 315,688 patient genomic profiles across 150 cancer types.
¶Commercially available qPCR methods were Roche cobas® EGFR mutation test v2 and Qiagen therascreen EGFR RGQ PCR kit.
Another notable issue is the accurate application of NGS data to clinical care. In multiple retrospective, observational cohort studies, approximately 17% to 24% of treatment-naive and 14% to 22% of second-line patients with EGFR exon 20 insertions received EGFR TKIs.11,17,22** Studies also found that approximately 7% to 40% of treatment-naive and 26% to 41% of second-line patients received IO monotherapy.17,22,23 These therapies (ie, most TKIs indicated for common mutations†† and IO monotherapies) are not recommended for first- or second-line therapy for EGFR exon 20 insertion mutations.5
**EGFR TKIs included first-, second- and third-generations.
††Exceptions include p.A763_Y764insFQEA and p.A763_Y764insLQEA.
Current Treatment Strategies for Patients With Exon 20 Insertion Mutations
Chemotherapy with a platinum doublet remains the recommended treatment option for the first-line treatment of patients with an EGFR exon 20 insertion mutation.5 When many of these patients progress, subsequent treatment options are needed. The NCCN Guidelines recommend amivantamab-vmjw or mobocertinib as subsequent therapy options for patients with EGFR exon 20 insertion mutations who have progressed on or after initial systemic therapy.5
Conclusion:
- Advances made in the treatment of NSCLC have improved patient mortality and survival,2 and these advancements are due in part to the discovery of actionable mutations, like common EGFR mutations, and targeted therapies3,4,7,8
- Multiple studies have found, however, that patients with EGFR exon 20 insertion mutations had a poor overall response when treated with first-, second-, or third-generation EGFR TKIs,11-15,17 and that IO monotherapies provide little benefit as a first-line treatment in patients with EGFR mutations, including exon 20 insertions17
- The NCCN Guidelines recommend:
- Testing eligible patients with mNSCLC for targetable genetic alterations to both identify potentially appropriate targeted therapies and avoid therapies unlikely to provide clinical benefit5
- Treating patients who harbor a common EGFR mutation (exon 19 deletion and exon 21 [L858R] mutations) with an EGFR TKI in the first line of treatment, whereas those with an EGFR exon 20 insertion mutation are best treated with a regimen containing a platinum doublet5
- Amivantamab-vmjw or mobocertinib as subsequent therapy options for patients with EGFR+ mNSCLC with exon 20 insertion mutations who have progressed on or after initial systemic therapy per the NCCN Guidelines5
References
1. National Cancer Institute. Cancer stat facts: common cancer sites. Accessed September 30, 2022. https://seer.cancer.gov/statfacts/html/common.html
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021.CA Cancer J Clin. 2021;71:7-33.
3. Benjamin DJ, Haslam A, Gill J, Prasad V. Targeted therapy in lung cancer: Are we closing the gap in years of life lost? Cancer Med. 2022;11(18):3417-3424.
4. Targeted Therapy in Metastatic Non–Small Cell Lung Cancer: Recent Updates and Controversies. Angel Qin. ASCO Daily News. Published January 19, 2022. Accessed November 14, 2022. https://dailynews.ascopubs.org/do/10.1200/ADN.22.200810/
5. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.6.2022. © National Comprehensive Cancer Network, Inc. 2022. All rights reserved. Accessed December 2, 2022. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in anyway.
6. Jordan EJ, Kim HR, Arcila ME, et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017;7(6):596-609.
7. Luo SY, Lam DC. Oncogenic driver mutations in lung cancer. Transl Respir Med. 2013;1(1):6.
8. Gazdar AF. Activating and resistance mutations of EGFR in non-small-cell lung cancer: role in clinical response to EGFR tyrosine kinase inhibitors. Oncogene. 2009;28 (Suppl 1):S24-S31.
9. Arcila ME, Nafa K, Chaft JE, et al. EGFR exon20 insertion mutations in lung adenocarcinomas: prevalence, molecular heterogeneity, and clinicopathologic characteristics. Mol Cancer Ther. 2013;12(2):220-229.
10. Leal JL, Alexander M, Itchins M, et al. EGFR exon 20 insertion mutations: clinicopathological characteristics and treatment outcomes in advanced non-small cell lung cancer. Clin Lung Cancer. 2021;22(6):e859-e869.
11. Bazhenova L, Minchom A, Viteri S, et al. Comparative clinical outcomes for patients with advanced NSCLC harboring EGFR exon 20 insertion mutations and common EGFR mutations. Lung Cancer. 2021;162:154-161.
12. Wu JY, Yu CJ, Shih JY. Effectiveness of treatments for advanced non-small-cell lung cancer with exon 20 insertion epidermal growth factor receptor mutations. Clin Lung Cancer. 2019;20:e620-e630.
13. Yang JC, Sequist LV, Geater SL, et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: a combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6.Lancet Oncol. 2015;16(7):830-838.
14. Kate S, Chougule A, JoshiA, et al. Outcome of uncommon EGFR mutation positive newly diagnosed advanced non-small cell lung cancer patients: a single center retrospective analysis. Lung Cancer (Auckl). 2019;10:1-10.
15. Kwon CS, Lin HM, Crossland V, et al. Non-small cell lung cancer with EGFR exon 20 insertion mutation: a systematic literature review and meta-analysis of patient outcomes. Curr Med Res Opin. 2022;38(8):1341-1350.
16. Robichaux JP, Elamin YY, Tan Z, et al. Mechanisms and clinical activity of an EGFR and HER2 exon 20-selective kinase inhibitor in non-small cell lung cancer. Nat Med. 2018;24:638-646.
17. Girard N, Minchom A, Ou SI, et al. Comparative clinical outcomes between EGFR ex20 ins and wild type NSCLC treated with immune checkpoint inhibitors. Clin Lung Cancer. 2022;23(7):571-577.
18. Paz-Ares L, Gondos A, Saldana D, et al. Genomic testing among patients with newly diagnosed advanced non-small cell lung cancer in the United States: A contemporary clinical practice patterns study. Lung Cancer. 2022;167:41-48.
19. Waterhouse DM, Tseng WY, Espirito JL, Robert NJ. Understanding contemporary molecular biomarker testing rates and trends for metastatic NSCLC among community oncologists. Clin Lung Cancer. 2021;22(6):e901-e910.
20. Robert N, Chen L, Espirito J, et al. Trends in molecular testing for metastatic non-small cell lung cancer in the US Oncology Network community practices. J Thorac Oncol. 2021;16(10) (suppl):S1169.
21. Bauml J, Viteri S, Minchom A, et al. Underdiagnosis of EGFR exon 20 insertion mutation variants: estimates from NGS-based real-world datasets. Presented at: the IASLC 2020 World Conference on Lung Cancer; January 28-31, 2021;Singapore.
22. He J, Pericone CD, Vanderpoel J. Real-world patient characteristics, treatment patterns, and mutation testing patterns among US patients with advanced non-small cell lung cancer harboring EGFR mutations. Adv Ther. 2022;39(7):3347-3360.
23. Choudhury NJ, Schoenfeld AJ, Flynn J, et al. Response to standard therapies and comprehensive genomic analysis for patients with lung adenocarcinoma with EGFR exon 20 insertions. Clin Cancer Res. 2021;27(10):2920-2927.
© Janssen Biotech, Inc. 2022 12/22 cp-345345v1
KRAZATI® (Adagrasib)
The FDA on December 12, 2022, granted accelerated approval to KRAZATI® (Adagrasib), a RAS GTPase family inhibitor, for adult patients with KRAS G12C-mutated locally advanced or metastatic Non-Small Cell Lung Cancer (NSCLC), as determined by an FDA-approved test, who have received at least one prior systemic therapy. KRAZATI® is a product of Mirati Therapeutics, Inc.
IMJUDO® (Tremelimumab)
The FDA on November 10, 2022, approved IMJUDO® (Tremelimumab) in combination with IMFINZI® (Durvalumab) and platinum-based chemotherapy for adult patients with metastatic Non-Small Cell Lung Cancer (NSCLC) with no sensitizing Epidermal Growth Factor Receptor (EGFR) mutation or Anaplastic Lymphoma Kinase (ALK) genomic tumor aberrations. Both IMJUDO® and IMFINZI® are products of AstraZeneca Pharmaceuticals.
LIBTAYO® (Cemiplimab-rwlc)
The FDA on November 8, 2022, approved LIBTAYO® (Cemiplimab-rwlc) in combination with platinum-based chemotherapy for adult patients with advanced Non-Small Cell Lung Cancer (NSCLC) with no EGFR, ALK, or ROS1 aberrations. LIBTAYO® is a product of Regeneron Pharmaceuticals, Inc.
RETEVMO® (Selpercatinib)
The FDA on September 21, 2022, granted regular approval to RETEVMO® (Selpercatinib) for adult patients with locally advanced or metastatic Non-Small Cell Lung Cancer (NSCLC) with a REearranged during Transfection (RET) gene fusion, as detected by an FDA-approved test. RETEVMO® is a product of Eli Lilly and Company.
Landmark Five Year Overall Survival Rates for OPDIVO® and YERVOY® Combination in Advanced NSCLC
SUMMARY: The American Cancer Society estimates that for 2022, about 236,740 new cases of lung cancer will be diagnosed and 135,360 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions by switching off the immune system T cells. Immune checkpoint proteins/receptors include CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4, also known as CD152) and PD-1(Programmed cell Death 1). Checkpoint inhibitors unleash the T cells resulting in T cell proliferation, activation, and a therapeutic response. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. YERVOY® is a fully human immunoglobulin G1 monoclonal antibody that blocks Immune checkpoint protein/receptor CTLA-4.
CheckMate-227 is an open-label, multi-part, global, Phase III trial in which OPDIVO® based regimens were compared with Platinum-doublet chemotherapy in patients with first line advanced NSCLC, across non-squamous and squamous tumor histologies. This study consisted of Part 1a/Part 1b and Part 2. In Part 2 of this trial, OPDIVO® plus chemotherapy was compared with chemotherapy alone, regardless of PD-L1 expression. Part 2 did not meet its Primary endpoint for Overall Survival for OPDIVO® plus chemotherapy versus chemotherapy alone, in patients with non-squamous NSCLC, and is published elsewhere.
Part 1a: Patients received OPDIVO® 3 mg/kg IV every 2 weeks plus YERVOY® 1 mg/kg IV every 6 weeks (N=396), OPDIVO® monotherapy 240 mg IV every 2 weeks (N=396) or chemotherapy alone given every 3 weeks for up to four cycles (N=397), in patients whose tumors had PD-L1 expression of 1% or more.
Part 1b: Patients received OPDIVO® plus YERVOY® (N=187), OPDIVO® 360 mg IV every 3 weeks plus chemotherapy IV every 3 weeks for up to four cycles (N=177), or chemotherapy alone IV every 3 weeks for up to four cycles (N=186), in patients whose tumors did not express PD-L1 (less than 1%)
Patients were stratified by histology, and treatment was administered until disease progression, unacceptable toxicity, or administered for 2 years for immunotherapy. It should be noted that when this trial was launched, chemotherapy along with immunotherapy or immunotherapy alone was not approved for the front-line treatment of NSCLC. Therefore, dual immunotherapy combination was not compared with current standards of care such as chemotherapy plus immunotherapy.
There were two independent Primary endpoints in Part 1 for OPDIVO® plus YERVOY® versus chemotherapy: Overall survival (OS) in patients whose tumors express PD-L1 (assessed in patients enrolled in Part 1a) and Progression Free Survival (PFS) in patients with TMB of 10 mut/Mb or more, across the PD-L1 spectrum (assessed in patients enrolled across Part 1a and Part 1b). Other assessments included Objective Response Rate (ORR), Duration of Response (DOR), and treatment-free interval. Treatment-free interval was measured in patients who discontinued study therapy and was defined as the time from last study dose to start of subsequent systemic therapy.
The Overall Survival (OS) data was previously reported at a minimum follow up of 29 months, and the median OS was of 17.1 months for the OPDIVO® plus YERVOY® group, compared to 14.9 months in the chemotherapy group (HR=0.79; P=0.007), with a 2-year OS rate of 40.0% and 32.8%, respectively. The researchers here in presented data after a minimum follow up of 61.3 months (5 years).
Patients whose tumors had PD-L1 expression of 1% or more continued to have sustained long term OS benefit with OPDIVO® plus YERVOY® when compared to chemotherapy (HR=0.77), and the 5-year OS rates were 24% with OPDIVO® plus YERVOY® compared to 14% with chemotherapy alone.
Patients with a PD-L1 expression of less than 1% also demonstrated continued long term OS benefit with OPDIVO® plus YERVOY® when compared to chemotherapy (HR = 0.65), and the 5-year OS rates were 19% for OPDIVO® plus YERVOY® compared to 7% for chemotherapy alone.
Among patients who survived for 5 years, median PFS was 59.1 months for PD-L1–positive patients and 60.7 months for PD-L1–negative patients who received OPDIVO® plus YERVOY®, compared to 9.5 months and 24.9 months respectively, for those who received chemotherapy.
Among those who responded to treatment, more patients who received OPDIVO® plus YERVOY® remained in response at five years, compared to chemotherapy, in both PD-L1 expression of 1% or more group (28% versus 3%) and PD-L1 expression of less than 1% group (21% versus 0%), respectively.
Among patients treated with OPDIVO® plus YERVOY® who were alive at five years, approximately two-thirds of patients did not receive any subsequent therapy for more than three years after stopping treatment, regardless of PD-L1 expression.
It was concluded that in this longest reported follow up of a Phase III trial of first line, chemotherapy free, combination immunotherapy, in metastatic Non Small cell Lung Cancer, a combination of OPDIVO® plus YERVOY® continued to provide long term durable clinical benefit and increased 5-year survivorship, when compared to chemotherapy, in previously untreated patients with metastatic NSCLC, regardless of PD-L1 expression.
Five-year survival outcomes with nivolumab (NIVO) plus ipilimumab (IPI) versus chemotherapy (chemo) as first-line (1L) treatment for metastatic non–small cell lung cancer (NSCLC): Results from CheckMate 227. Brahmer JR, Lee J-S, Ciuleanu T-E, et al. DOI: 10.1200/JCO.22.01503 Journal of Clinical Oncology. Published online October 12, 2022.
FDA Grants Accelerated Approval to KRAZATI® for KRAS G12C-mutated NSCLC
SUMMARY: The FDA on December 12, 2022, granted accelerated approval to KRAZATI® (Adagrasib), a RAS GTPase family inhibitor, for adult patients with KRAS G12C-mutated locally advanced or metastatic Non-Small Cell Lung Cancer (NSCLC), as determined by an FDA-approved test, who have received at least one prior systemic therapy. FDA also approved the QIAGEN therascreen KRAS RGQ PCR kit (tissue) and the Agilent Resolution ctDx FIRST Assay (plasma) as companion diagnostics for KRAZATI®. If no mutation is detected in a plasma specimen, the tumor tissue should be tested.
The American Cancer Society estimates that for 2022, about 236,740 new cases of lung cancer will be diagnosed and 135,360 patients will die of the disease. Lung cancer is the leading cause of cancer-related mortality in the United States. Non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of NSCLC, 30% are Squamous Cell Carcinomas (SCC), 40% are Adenocarcinomas and 10% are Large Cell Carcinomas. With changes in the cigarette composition and decline in tobacco consumption over the past several decades, Adenocarcinoma now is the most frequent histologic subtype of lung cancer.
The KRAS (kirsten rat sarcoma viral oncogene homologue) proto-oncogene encodes a protein that is a member of the small GTPase super family. The KRAS gene provides instructions for making the KRAS protein, which is a part of a signaling pathway known as the RAS/MAPK pathway. By relaying signals from outside the cell to the cell nucleus, the protein instructs the cell to grow, divide and differentiate. The KRAS protein is a GTPase and converts GTP into GDP. To transmit signals, the KRAS protein must be turned on by binding to a molecule of GTP. When GTP is converted to GDP, the KRAS protein is turned off or inactivated, and when the KRAS protein is bound to GDP, it does not relay signals to the cell nucleus. The KRAS gene is in the Ras family of oncogenes, which also includes two other genes, HRAS and NRAS. When mutated, oncogenes have the potential to change normal cells cancerous.
KRAS is the most frequently mutated oncogene in human cancers and are often associated with resistance to targeted therapies and poor outcomes. The KRAS G12C mutation occurs in approximately 25% of Non-Small Cell Lung Cancers (NSCLC) and in 3-5% of colorectal cancers and other solid cancers. KRAS G12C is one of the most prevalent driver mutations in NSCLC and accounts for a greater number of patients than those with ALK, ROS1, RET, and TRK 1/2/3 mutations combined. KRAS G12C cancers are genomically more heterogeneous and occur more frequently in current or former smokers and are likely to be more complex genomically than EGFR mutant or ALK rearranged cancers. G12C is a single point mutation with a Glycine-to-Cysteine substitution at codon 12. This substitution favors the activated state of KRAS, resulting in a predominantly GTP-bound KRAS oncoprotein, amplifying signaling pathways that lead to oncogenesis.
KRAZATI® (Adagrasib) is a potent, orally available, small molecule covalent inhibitor of KRAS G12C. This drug irreversibly and selectively binds KRAS G12C in its inactive, GDP-bound state. Unlike LUMAKRAS® (Sotorasib), which is also a selective covalent inhibitor of KRAS G12C, KRAZATI® has a longer drug half-life of 23 hours, as compared to 5 hours for LUMAKRAS®, has dose-dependent extended exposure, and can penetrate the CNS. Approximately, 27-42% of patients with NSCLC harboring KRAS G12C mutations have CNS metastases, with poor outcomes. KRYSTAL-1 is a Phase I/II multiple expansion cohort trial involving patients with advanced solid tumors harboring a KRAS G12C mutation. KRAZATI® demonstrated clinical activity in patients with KRAS G12C-mutated solid tumors, including colorectal, pancreatic, and biliary tract cancers. Further, preliminary data from two patients with untreated CNS metastases from a Phase 1b cohort showed antitumor activity against CNS metastases, with satisfactory concentrations of KRAZATI® in the CSF.
The present FDA approval was based on the results from Cohort A, a Phase 2 cohort of the KRYSTAL-1 study in which KRAZATI® at a dose of 600 mg orally twice daily was evaluated in patients with KRAS G12C-mutated NSCLC, previously treated with chemotherapy and anti-Programmed Death 1 (PD-1) or Programmed Death Ligand 1 (PD-L1) therapy. This registration study included a total of 116 unresectable or metastatic NSCLC patients, with histologically confirmed diagnosis, with KRAS G12C mutation (detected in tumor tissue at a local or central laboratory), who had previously received treatment with at least one platinum-containing chemotherapy regimen and checkpoint inhibitor therapy (in sequence or concurrently), and who had measurable tumor lesions. Enrolled patients received KRAZATI® 600 mg capsule twice daily, and treatment was continued until disease progression or unacceptable toxicities. The median patient age was 64 years, 97% had adenocarcinoma histology, 98% had both platinum-based therapy and checkpoint inhibitor therapy, and 21% of patients had CNS metastases. Key exclusion criteria included active CNS metastases (patients were eligible if CNS metastases were adequately treated and neurologically stable), carcinomatous meningitis, and previous treatment with a KRAS G12C inhibitor. Exploratory Biomarker Analyses included candidate biomarkers (PD-L1 Tumor Proportion Score and mutational status of STK11, KEAP1, TP53, and CDKN2A on tumor-tissue specimens, blood specimens, or both, for their association with tumor response. The Primary end point was Objective Response Rate as assessed by blinded Independent Central Review. Secondary end points included the Duration of Response, Progression Free Survival, Overall Survival, and safety. The median follow up was 12.9 months and the median duration of treatment was 5.7 months.
Of 112 patients with measurable disease at baseline, the confirmed Objective Response Rate was 42.9% and the median Duration of Response was 8.5 months. The median Progression Free Survival was 6.5 months, and the median Overall Survival was 12.6 months, at a median follow up of 15.6 months. Among 33 patients with previously treated, stable CNS metastases, the intracranial confirmed Objective Response Rate was 33.3%. Treatment-related adverse events occurred in 97.4% of the patients and 53% were Grade 1 or 2 toxicities. KRAZATI® was discontinued in 6.9% of patients due to adverse events.
It was concluded that among patients with previously treated KRAS G12C-mutated NSCLC, KRAZATI® showed significant clinical efficacy without new safety signals and encouraging intracranial activity. The researchers added that these are the first clinical data demonstrating CNS-specific activity of a KRAS G12C inhibitor in this patient population.
Adagrasib in Non–Small-Cell Lung Cancer Harboring a KRASG12C Mutation. Jänne PA, Riely GJ, Gadgeel SM, et al. N Engl J Med 2022; 387:1238-1239